
Until just a few weeks ago, here is everything I knew about my sinuses:
1. They are inside my head.
2. They are usually clogged with horrible mucus.
3. The horrible mucus leaks out of my nostrils.
4. Sinuses are disgusting, and the less time spent thinking about them the better.
• • •
Or so I thought.
It turns out that modern medicine is mind-blowing, and I mean that in a thoroughly positive way. I might have meant it otherwise had my doctor’s hand somehow slipped during surgery, but that’s getting well ahead of the story.
For now, here’s what you need to know:
After fifty years of inadequate breathing, decades of pulsing discomfort, a general sense of “I hate my sinuses, why do I even have them,” I was informed by modern medicine, in the form of a young, slender, oddly confident ENT specialist, that my problem was not my sinuses per se, but sinus polyps—grape-sized blobs of I-don’t-know-and-I-didn’t-ask.
These grape-sized blobs of I-don’t-know-and-I-didn’t-ask are what kept my sinuses from filling with air. They also kept them from flushing out all the horrible mucus. Thus: infection, pain, poor breathing, infection, gunk, embarrassment, infection, more pain, a box of Kleenex on every flat surface of my home, burning, swelling, infection, pain. Repeat cycle once each month.
Then modern medicine suggested: “We can clear those out.”
"How?” I asked.
“Well, we go up through the nostrils . . .” the doctor said.
“The nostrils, you say?”
“Yes,” the young physician answered, and then he offered a sentence that contained the word “scraping,” and I removed myself from all conscious comprehension for about ten seconds, until he said, “Of course, we wouldn’t want to scrape too much, because the bone separating your sinuses from your brain is very thin.”
As I said: Potentially mind-blowing.
It was at that juncture that I stopped listening for about thirty seconds, until the doctor added, “So we should probably schedule this up in Columbus, just to be on the safe side.”
I remember wondering why the thin layer of bone separating my sinuses from my brain would be less likely to perforate catastrophically in Columbus, the capital of Ohio, about eighty miles upstream from the small college town where my sinuses usually clog themselves. But it didn’t take long before the doctor said, “Imaging.”
“Oh,” I nodded, trying to look respectful and informed. “Who’s Imogene?”
• • •
So, here are six actual facts I didn’t know about my sinuses before Doctor Gallant (not his real name, but it should be) entered the picture:
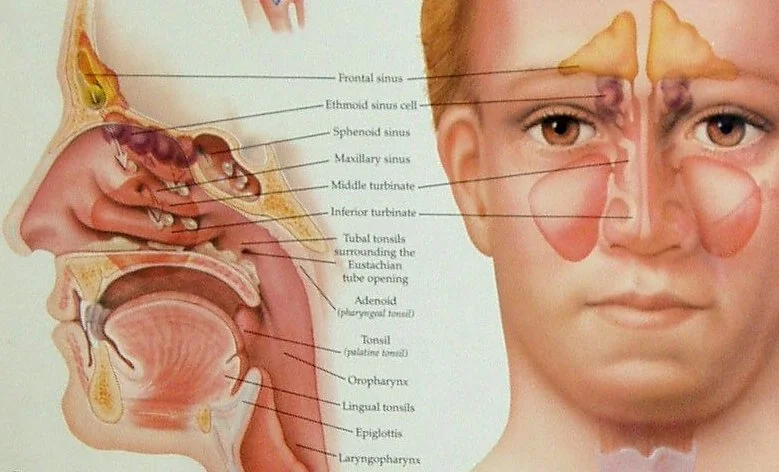
1. There are not two but four sinus cavities in the skull—one on either side of the nose, but also one above each eye, behind the eyebrow.
2. Scientists can’t agree why these openings exist.
3. One theory is that they decrease the weight of the skull, making it easier to hold up our heads all day.
4. Another theory is that they act as shock absorbers, decreasing injury when the head hits something harder than a pillow.
5. The goop we all despise exists for good reason: to capture viruses, bacteria, and other airborne particles before they reach our lungs.
6. When we are sick, mucus production can increase to two liters a day. Think two-liter Pepsi bottle, and then get entirely grossed out.
• • •
There was, it turns out, no Imogene.
Dr. Gallant scheduled me in early August for Computer-Assisted Endoscopic Sinus Surgery. This involved the insertion of a very thin, fiber-optic scope into my nose and the use of micro instruments (aka “scrapers”) to remove the little grape-sized blobs of I-didn’t-ask. Of course, if the doctor was going to wander around with tiny X-ACTO knives, it would be good for him to see where he was scraping. The hospital in Columbus, it turns out, had imaging technology.
First, though, I had to get medically cleared for the operation. Because I am in advanced middle age, I have many doctors; we humans accumulate them like barnacles attached to an aging frigate. None of my many doctors, of course, could figure out how to share information with any of my other many doctors, including doctors whose offices are one floor apart in the same medical complex. “I can just walk it down,” I would say, but they had protocols, and costly computer systems that couldn’t talk to one another, or do anything really, except billing.
The billing always worked.
Nonetheless, August rolled around, and I presented myself at the Outpatient Surgery Center, located just a few blocks from the enormous university teaching hospital, and all was well, except at the last minute I mentioned that I’d recently been diagnosed with sleep apnea, a Greek word that allows doctors to bill you at two-hundred-times the rate they might if we just called it snoring.
My procedure was delayed while the medical team endeavored to learn my sleep apnea score, which somehow had never found its way into any of my voluminous medical records.
“I believe I scored well,” I said, which didn’t satisfy the anesthesiologist’s curiosity at all.
Sixteen computers in sixteen different medical offices spread across most of southern Ohio refused to speak to one another for a good bit of the morning, until the resourceful anesthesiologist finally just picked up his cell phone and dialed.
The last voice I heard before succumbing to the happy gas was the masked cell-phone user reacting to the score he was given:
“Holy cow!”
• • •
I assume the doctor has wonderful memories of touring the folds and caverns behind my facial bones, but since Gallant and his team kept me sedated and oblivious, my only way of describing what occurred is to watch similar procedures on YouTube, where, it turns out, hundreds of doctors have recorded thousands of excruciating hours of footage revealing just about any medical technique you might want to watch. It is creepy, to be honest, because the doctors in these videos talk animatedly at the camera for most of the operation, and I keep wanting to shout, “Oh my God, focus on the patient, focus on the patient!”
The online videos of Computer-Assisted Endoscopic Sinus Surgery using image guidance aren’t pretty, believe me. The flexible tube inserted through the nostril contains both a light source and a camera, and the inner walls, gooey corners, and grape-sized I-don’t-know-whats are revealed on a TV monitor. The videos look like outtakes from a movie entitled Journey to the Center of an Astonishingly Gross Earth, or perhaps extremely poor-quality porn, shot way too close up.
• • •
I awoke from my procedure feeling quite chipper. Until Dr. Gallant and the anesthesiologist informed me I would not be heading home as planned, but staying the night in a local hospital. My “holy cow!” sleep apnea score, they concluded, combined with the amount of anesthesia it took to knock me out for surgery, risked that unpleasant moment where my airwaves would briefly shut off breathing, and my reflexes would just roll over and say, “Oh don’t wake us now, we’re having such a nice dream.”
In other words, I would asphyxiate.
The medical chaps, as they loved to say over and over again, decided to “exercise a little extra caution.”
This did not sit well with me. I wanted to recover at home, as “outpatient” surgery suggested, both because of sentimental reasons, but also because I had planned my “at home” outpatient recovery in exquisite detail, a sort of one-man New Year’s Eve celebration featuring cold beer, junk television, nose bandages, and pain killers. What could go wrong?
I wasn’t going to find out because I wasn’t going home, which was bad enough. Worse yet was when the hospital reported having no open rooms.
The real problem was that I felt absolutely fine. Anesthesia has the odd effect of energizing me immediately after awakening, rather than leaving me drowsy, but given my “post-op” status, I was stuck with two choices—either lie on my back and complain, or sit up just a little, sip water, and complain.
Three hours of this, until finally I was cleared for a room in the hospital six blocks away, and then—yes, only then—a nurse informs me that an ambulance has been called, and that will take “. . . about three more hours.”
“Your case is not urgent,” she added.
What I said in response may not have been polite, and I hereby apologize to anyone anywhere who has ever worked in the medical care profession.
About this point, I went to work trying to convince the nursing staff that I easily enough could walk the six blocks to the hospital. Or I could drive, if they lent me a car. Or one of them could drive me, and I’d buy ice cream on the way.
Miraculously, and to the boundless relief of the nurses, my ambulance arrived a full hour and-a-half early, and I was quickly strapped in, attached to four thousand wires, monitoring every inch of my body except perhaps my nose, where I believe the surgery had been performed. And then, finally, I was driven the three-minutes’ distance from the surgery center to the medical center, at about twenty miles per hour, no lights, no siren.
At one point, concerned that her patient might be disoriented by this wild ride, the med tech in the back asked me the name of the current president.
“Sarah Palin,” I answered, hoping to exhibit the fine nuance of my post-operative intellectual irony.
“Ha!” she answered with no hint of humor. “Don’t we wish.”
• • •
Faster than one can say Affordable Care Act, I was whisked into my room, on the hospital’s fifth floor. The man in the bed across from me was glad for company, because he had quite the story to tell, one I heard about eight times in the next four hours.
Mr. Deeter was from Akron, and his job, he told me, was to service giant transformers, the ones you see along the roadside surrounded by ten-foot cyclone fencing with signs reading: “High Voltage! Do Not Enter!”
Mr. Deeter regularly ignored those signs—it was, in fact, his job to do so. That morning he had been pulling oil from the engine of one of these powerful transformers, “with a syringe,” he shouted across the two beds, “the way a nurse takes blood”—when his bare arm touched something it should not have touched, and 81,000 volts of electricity coursed through his body.
“I let out a yelp,” he told me. “And BAM! Next thing I knew I was knocked back up against the fence.”
He stopped for a moment, studied my face. What he saw was an expression that best translates as, “And you lived?”
Mr. Deeter seemed to be rounding sixty or so, with a short, military haircut, the fit physique of a man who works outside with tools, and a deep, no-nonsense voice. He was proud of his ability to survive the massive burst of voltage, or maybe he was still in shock. Either way, he repeated his story to everyone who entered the room.
“Couldn’t feel my arm at first, so I looked down, and, yup, it was still attached.” He would pause here for effect. “Then I went back to work, siphoning out the oil. I noticed this burn on my elbow, and thought, ‘Oh nuts! I guess I should call this one in.’ But I didn’t.”
Turned out Mr. Deeter had two small, round burns: one on his elbow, just an inch or so from where his safety gloves ended, and one on his chest, where the voltage apparently surged back out of his body.
He didn’t call to report the accident until a co-worker showed up, and said, “Deeter, you don’t look so good.”
“He was right. I called it in. Now I’m here.”
He didn’t look like a man shot through with electricity. He looked fine, as fine as I felt. He also looked trapped, like he’d rather be anywhere, even back servicing generators, than in that hospital room.
I knew exactly how he felt.
• • •
Scientists, as I said earlier, can’t agree on why we have sinuses.
The make-our-heads-lighter-so-we-can-holdthem-erect notion has its staunch advocates, as does the shock-absorber-in-the-skull idea, but, hands-down, my favorite theory posits that we—you, me, Mr. Deeter, and Sarah Palin alike—are descended from aquatic apes.
The theory goes like this: a group of prehistoric primates, cleverer than most, noticed that river banks and sea shores produced much better food than did arid grasslands, so they descended from their treetops and acquired waterfront property.
Over time, through the exquisite magic of evolution, these apes evolved an upright stance, allowing them to stand in the water and freeing up their hands to crack shellfish. Eventually they also lost their body hair, developing instead a thick layer of subcutaneous fat (to keep warm in the water). They learned to swim.
And this, if you believe Peter Rhys Evans, a British expert on head-and-neck physiology, also explains our sinus cavities.
Compared to other primates, humans have particularly large openings in the skull, Rhys Evans notes. “It makes no sense until we consider the evolutionary perspective. Then it becomes clear: our sinuses acted as buoyancy aids that helped keep our heads above water.”
He adds further evidence: unlike our ape cousins, humans have an unusually strong diving reflex, a unique nose shape that shields our nostrils when we dive below the surface, and partial webbing between our fingers and toes.
Not all scientists agree, because if they did, how could they write hundreds of scholarly articles arguing over every detail—but a good many do agree. And who doesn’t like a spirited squabble over how primeval monkeys transformed themselves over time into twenty-first-century hipsters wearing skinny jeans and taking selfies?
Turns out, it all started at the oyster bar.
• • •
Why exactly do human beings have unique tongue prints?
Why do we have that vertical groove on the surface of our upper lip?
What’s the meaning of goosebumps?
What purpose does the uvula serve, and why does it sound so dirty?
If Mr. Deeter could absorb thousands of volts of electricity through his arm and shoot it back out of his chest, sustaining little more than a few surface burns, and then go back to work for thirty minutes before deciding to call his supervisor, why can’t monkeys evolve large open spaces in their skulls to keep their heads above water as they float down the lazy river, popping tasty minnows into their hungry mouths?
I’m talking about the glorious mystery of the body here, which might sound like a pickup line, but I don’t mean it that way.
Goosebumps, by the way, occur when tiny muscles around the base of each hair tense, pulling the hair more erect. Back when we were apes, our fur would stand on end, to make us look larger, scarier, more powerful. Now, we just look silly.
Our bodies, even our sinuses, are simply miraculous. I’ve progressed from hating my goopy head cavities to being damned proud of them.
They exist for a reason.
A good reason.
They exist because somehow, somewhere in time, an ape looked around and thought, “Man, you know what I could go for right now? Shrimp cocktail.”
Dinty W. Moore lives in Athens, Ohio, the funkadelicious, hillbilly-hippie Appalachian epicenter of the locally-grown, locally-consumed, goats-are-for-cheese, paw-paws-are-for-eatin’, artisanal-salsa, our-farmers-market-rocks-the-hills sub-culture, where he grows his own heirloom tomatoes and edible dandelions, and teaches a crop of brilliant undergraduate and stunningly talented graduate students as director of Ohio University’s BA, MA, and PhD in Creative Writing program. He has been published in The Southern Review, The Georgia Review, Harpers, The New York Times Sunday Magazine, The Philadelphia Inquirer Magazine, Gettysburg Review, Utne Reader, Crazyhorse, and Okey-Panky, among numerous other venues. He has authored several books, including Dear Mister Essay Writer Guy: Advice and Confessions on Life, Love, and Cannibals and The Story Cure: A Book Doctor's Pain-Free Guide to Finishing Your Novel or Memoir.
Photo on Foter.com